Element 4: Develop a comprehensive care plan
A documented comprehensive care plan (or plan for care) reflects shared decisions made with patients, carers and families about the tests, interventions, treatments and other activities needed to achieve the goals of care.
A single plan (one document or digital view) is not a requirement. However, each patient should have a comprehensive plan for care developed relevant to their care needs. The plan for care should allow for core information to be easily shared, accessed and acted on by all members of the multidisciplinary team. The plan for care can be documented on paper or in electronic form.
Action 5.13 states:
Clinicians use processes for shared decision making to develop and document a comprehensive and individualised plan that:
- Addresses the significance and complexity of the patient’s health issues and risks of harm
- Identifies agreed goals and actions for the patient’s treatment and care
- Identifies the support people a patient wants involved in communications and decision-making about their care
- Commences discharge planning at the beginning of the episode of care
- Includes a plan for referral to follow-up services if appropriate and available
- Is consistent with best practice and evidence.
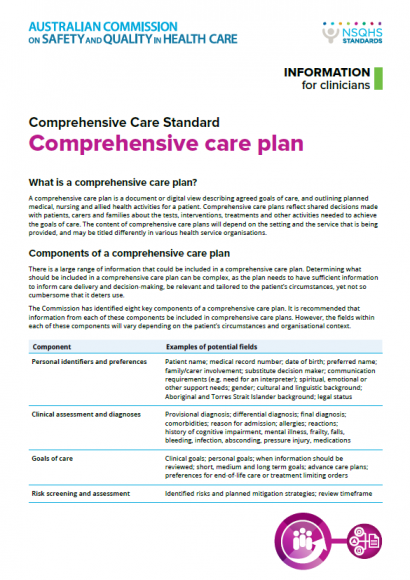
Diagnoses, risk screening and clinical assessment findings inform the comprehensive care plan.
Resources
The Commission has developed resources providing guidance on the type of information that could be included in a comprehensive care plan.