Surveillance of Clostridioides difficile infection
Continuous, ongoing surveillance of Clostridioides difficile infection (CDI) in hospitals contributes to safer care for patients and informs strategies to improve practice and minimise rates of preventable CDI.
Implementation Guide
This guide supports Australian health service organisations to implement surveillance of hospital-identified Clostridioides difficile infection (CDI) and contribute to national reporting. Criterion B1 of the CDI case definition was updated in August 2024 to include testing for CDI toxin gene(s) and ensure consistency with the current Public Health Laboratory Network CDI laboratory case definition.
Case definition – Hospital-identified CDI
A hospital-identified CDI case is a case of CDI identified for a patient attending a hospital (including positive specimens obtained from admitted patients and those attending the emergency department, and outpatient departments). This does not mean the case of CDI is attributed to or acquired at the hospital conducting the surveillance.
A case of CDI implies that the patient has the relevant clinical manifestations and must meet either: 1) Criterion A and either Criterion B1 or B2; or 2) Criterion A and Criterion C.
A case of hospital-identified CDI:
| A | B1 | B2 | C |
|---|---|---|---|
| X | X | ||
| X | X | ||
| X | X |
Not a case of hospital-identified CDI:
| A | B1 | B2 | C |
|---|---|---|---|
| X | |||
| X | |||
| X |
Criterion A:
Diarrhoea (usually defined as three or more loose stools in a 24-hour period) or, less commonly, ileus, toxic megacolon or pseudomembranous colitis (identified by colonoscopy).
AND EITHER
Microbiological evidence of toxin producing C. difficile from at least one of the following criteria:
Criterion B1:
Positive laboratory test result for C difficile toxin A and or B or toxin gene(s) tested on an unformed diarrhoea) stool specimen.
OR
Criterion B2:
A toxin-producing C. difficile organism detected by culture or other laboratory means performed on an unformed stool sample.
OR
Criterion C:
Patient has evidence of pseudomembranous colitis on gross anatomic (includes endoscopic exams) or histopathologic exam.
Exclusions:
- Cases where a known previous positive test has been obtained within the last eight weeks
- Patients less than two years old at date of admission.
For guidance on testing procedures for C. difficile see the Public Health Laboratory Network. Clostridium difficile infection laboratory case definition.
Calculation of CDI rates
The following formula should be used to calculate the rate of C. difficile infection in acute inpatient hospitals:
| Numerator: | Patient episodes of hospital identified CDI (total hospital CDI cases) | x 10,000 |
|---|---|---|
| Denominator: | Number of patient days |
A hospital’s CDI rate should be calculated routinely as per the local surveillance plan. For example, on a monthly or quarterly basis to enable early outbreak detection and ongoing evaluation of the local infection control program.
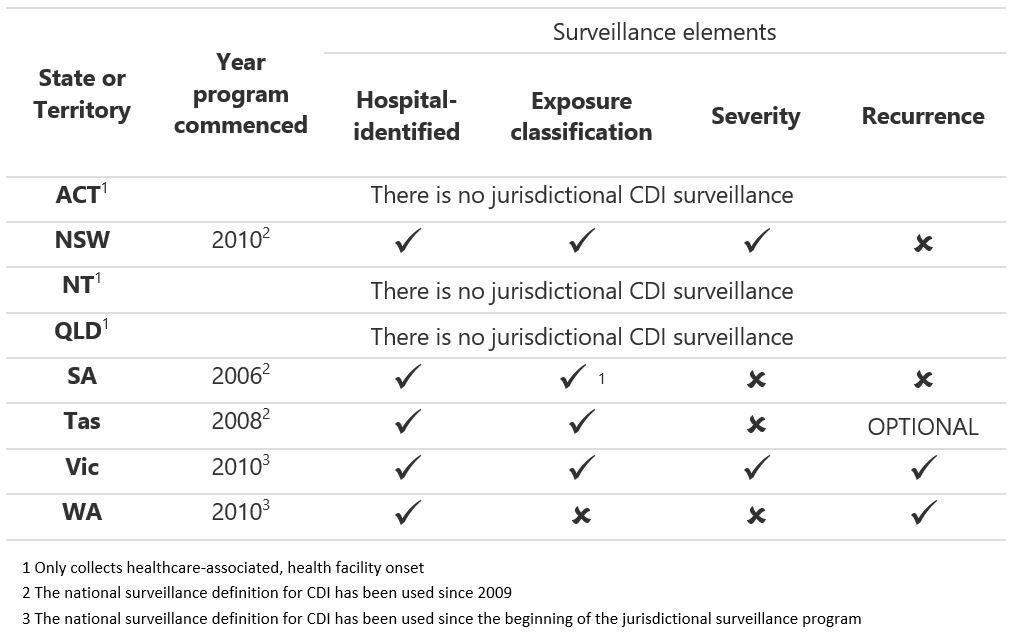
State CDI surveillance programs
Current state and territory CDI surveillance programs are summarised below: