Codes that can be used to identify patients diagnosed with sepsis from routinely collected data.

A reasonable adjustment is a change to an existing approach or process which is essential to ensure a person’s access to a service. Making reasonable adjustment for a person’s disability creates an inclusive environment and facilitates meeting the NSQHS Standards.
Information for healthcare services to guide practice and monitor improvement using the clinical care standard, and resources to support implementation.
The Sepsis Clinical Care Standard describes the health care that should be provided to patients with signs and symptoms of sepsis. It also addresses the care that should be provided in hospital and after discharge, including survivorship.
Guidance for clinicians on the seven quality statements from the Sepsis Clinical Care Standard, as well as helpful resources.
A patient who has survived sepsis receives individualised follow-up care to optimise functional outcomes, minimise recurrence, reduce rehospitalisation and manage the ongoing health effects of sepsis. This requires structured, holistic and coordinated post-discharge care and education that involves the patient, their family, carer, general practitioner and other clinicians.
Support and information are provided to the family or carer of a patient who has died from sepsis.
A patient with known or suspected sepsis has a documented clinical handover at transitions of care. This includes the provisional sepsis diagnosis, comorbidities, and the management plan for medicines and medical conditions. This information is provided to the patient, their family and carer as appropriate.
A patient, their family or carer is informed about sepsis from the time that it is suspected in a way that they can understand. Information includes the expected treatment and potential health effects of sepsis. Information is provided verbally and in writing.
A patient with suspected sepsis has blood cultures taken immediately, ensuring that this does not delay the administration of appropriate antimicrobial therapy. When signs of infection-related organ dysfunction are present, appropriate antimicrobials are started within 60 minutes. Antimicrobial therapy is managed in line with the Antimicrobial Stewardship Clinical Care Standard, including a review within 48 hours from the first dose.
Sepsis is a time-critical medical emergency. Assessment and treatment of a patient with suspected sepsis are started urgently according to a locally approved clinical pathway, and their response to treatment is monitored and reviewed. The patient is reviewed by a clinician experienced in recognising and managing sepsis, and is escalated to a higher level of care when required.
A diagnosis of sepsis is considered in any patient with an acute illness or clinical deterioration that may be due to infection. A clinical support tool that includes assessment of vital signs and lactate is used to help recognise sepsis early and escalate care when required.
The standard has been endorsed by a number of key professional associations and health organisations. Its development was supported by the Sepsis Clinical Care Standard Topic Working group.
The Australian Hospital Patient Experience Question Set has been translated into 20 languages, and is available in easy English, large print and braille.
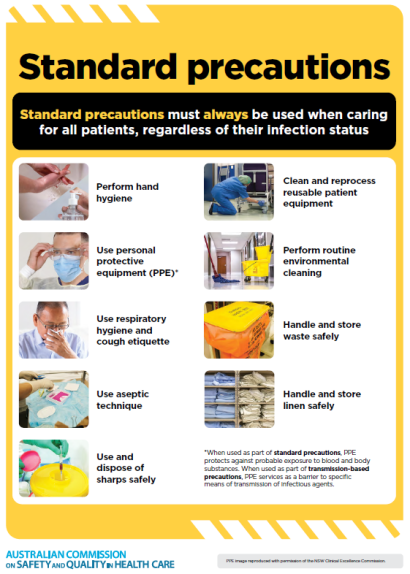
Aseptic technique is an element of standard precautions. Aseptic technique is a set of practices that protects patients from healthcare-associated infections and protects healthcare workers from contact with blood, body fluid and body tissue.
Not all actions within the Primary and Community Healthcare Standards will be applicable to every primary and community healthcare service.