Infection surveillance and monitoring
Monitoring infections that patients can get while receiving healthcare (known as healthcare-associated infections or HAIs) is an important way to improve patient safety.
HAI surveillance programs help hospitals check how well their current infection prevention and control practices are working and inform clinicians on how they can improve the way they work and achieve better outcomes for patients.
Surveillance for Staphylococcus aureus bloodstream infection (SABSI)
Monitoring Staphylococcus aureus bloodstream infections (SABSI) helps hospitals understand how well their infection prevention and control practices are working. SABSI rates are used across Australia as a key measure of hospital safety and quality.
Why SABSI surveillance matters
SABSI can cause serious illness and even death. Tracking where and why these infections occur helps hospitals to:
- Identify risk areas and high-risk procedures
- Improve infection prevention practices
- Monitor progress over time
- Provide timely feedback to clinicians about their own clinical practice
- Reduce preventable infections and improve patient outcomes.
National data on healthcare associated SABSI are published by the Australian Institute for Health and Welfare on the MyHospitals website, and states and territories may also publish their own data.
National monitoring and reporting
National benchmark for SABSI
Australia has a national benchmark to measure SABSI in public hospitals.
The current benchmark is 1.0 per 10,000 patient days. This benchmark took effect on 1 July 2020, replacing the previous limit of 2 per 10,000 patient days, and provides a consistent standard to support reliable monitoring and reporting across the country.
Case definition - what counts as a SABSI?
A patient episode of a SABSI is a positive blood culture for Staphylococcus aureus (S. aureus).
For surveillance purposes, only the first isolate per patient is counted, unless at least 14 days has passed without a positive culture, after which a subsequent episode is recorded.
A SABSI is healthcare-associated if Criterion A1 or A2, or Criterion B1, 2, 3 or 4 are met.
Criterion A
The patient’s first Staphylococcus aureus positive blood culture was collected:
- A1. More than 48 hours after admission, with no documented evidence that infection was present (including incubating) on admission
OR - A2. Less than 48 hours after discharge.
Criterion B
The patient’s first positive Staphylococcus aureus blood culture was collected less than or equal to 48 hours after admission and one or more of the following key clinical criteria is met:
- B1. SABSI is a complication of the presence of an indwelling medical device
- B2. SABSI occurs within 30 days of a surgical procedure where the SABSI is related to the surgical site, or 90 days for deep incisional/organ space infections related to a surgically implanted device
- B3. SABSI was diagnosed within 48 hours of a related invasive instrumentation or incision
- B4. SABSI is associated with neutropenia* contributed to by cytotoxic therapy and is unrelated to the presence of an indwelling medical device.
If neither Criterion A1 or 2, nor Criterion B1, 2, 3 or 4 are met, then the SABSI is considered to be community-acquired for the purposes of surveillance.
*Neutropenia is defined as at least two separate calendar days with values of absolute neutrophil count (ANC) or total white blood cells count (WBC).
Implementation guides and resources
To help hospitals collect and report SABSI data consistently, we have produced:
- Implementation Guide for the Surveillance of Staphylococcus aureus bloodstream infection
- Summary of changes – 2021 Implementation Guide for the Surveillance of Staphylococcus aureus Bloodstream Infection
A detailed SABSI data set specification is available in METeOR, the national data standards repository. This provides guidance for local data collection systems.
Surveillance for central line-associated bloodstream infection
Case definition – what counts as a CLABSI?
- A central line-associated bloodstream infection (CLABSI) is a laboratory-confirmed bloodstream infection in a patient where the central line was in place for >48 hours on the date of the event.*
AND - The central line was in place on the date of the event or the day before. If the central line was in place for >48 hours and then removed, the CLABSI criteria must be fully met on the day of discontinuation or the next day.
CLABSI must meet one of the following criteria:
Criterion 1
- A patient of any age has a recognised bacterial or fungal pathogen cultured from one or more blood cultures
AND - The organism cultured from blood is not related to an infection at another site.
OR
Criterion 2
- A patient of any age has at least one of the following signs or symptoms: fever (> 38°C), chills or hypotension
OR - A patient < 1 year of age has at least one of the following signs or symptoms: fever (> 38°C core), hypothermia (< 36°C core), apnoea or bradycardia
AND
The organism cultured from blood is not related to an infection at another site
AND
The same (matching) potential contaminant organism is cultured from two or more sets of blood cultures drawn on separate occasions within 24 hours.
Criterion elements, such as positive blood cultures and fever, must occur within a seven - day timeframe (the three days before and the three days after) the day on which the positive blood culture was drawn.
The same (matching) potential contaminant organisms† represent a single element of any of the criteria. The collection date of the first positive blood culture should be used to determine the date of the event.
Notes:
- *The Centers for Disease Control (CDC)/National Hospital Safety Network (NHSN) and some Australian states and territories use calendar days (>2 calendar days) as the metric for the duration of central line placement, with device placement being Day 1. A consistent metric must be used, whether it is hours or days.
- † Potential contaminant organisms (referred to as common commensals by the NHSN) include: diphtheroids [Corynebacterium spp. not C. diphtheria], Bacillus spp. [not B. anthracis], Propionibacterium spp., coagulase negative staphylococci [including S. epidermidis], viridans group streptococci, Aerococcus spp., Micrococcus spp., and Rhodococcus spp.
Implementation guides and resources
Most states and territories in Australia have voluntary or mandatory reporting systems in place for monitoring for CLABSI. To support this, the Commission have developed resources to help hospitals apply consistent methods for tracking CLABSI and improving patient safety.
- Implementation Guide: Surveillance of Central-Line Associated Bloodstream Infection (2019)
- Infographic - CLABSI Guide 2019
Surveillance of Clostridioides difficile infection
Continuous, ongoing surveillance of Clostridioides difficile infection (CDI) in hospitals helps keep patients safe and guides improvements in patient care.
This CDI surveillance guide helps health service organisations carry out surveillance of hospital identified CDI and supports national reporting. In August 2024, Criterion B1 of the CDI case definition was updated to include testing for CDI toxin genes, aligning it with the current Public Health Laboratory Network CDI laboratory case definition.
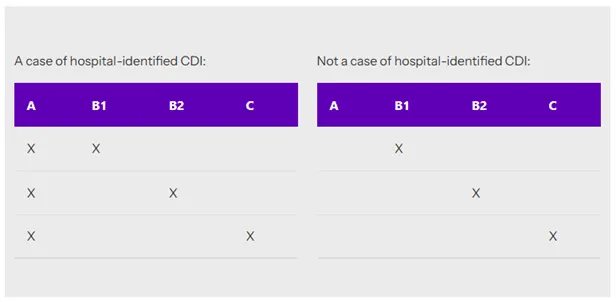
Case definition - Hospital-identified CDI
A hospital-identified CDI case is a case of CDI identified for a patient attending a hospital (including positive specimens obtained from admitted patients and those attending the emergency department, and outpatient departments). This does not mean the case of CDI is attributed to or acquired at the hospital conducting the surveillance.
A case of CDI requires relevant clinical manifestations and must meet:
- Criterion A AND Criterion B1 OR Criterion B2
OR - Criterion A AND Criterion C
Criterion A (required)
Diarrhoea (usually defined as three or more loose stools in a 24-hour period) or, less commonly, ileus, toxic megacolon or pseudomembranous colitis (identified by colonoscopy).
Microbiological evidence of toxin producing C. difficile from at least one of the following criteria:
Criterion B1:
Positive laboratory test result for C difficile toxin A and or B or toxin gene(s) tested on an unformed diarrhoea) stool specimen.
OR
Criterion B2:
A toxin-producing C. difficile organism detected by culture or other laboratory means performed on an unformed stool sample.
OR
Criterion C:
Patient has evidence of pseudomembranous colitis on gross anatomic (includes endoscopic exams) or histopathologic exam.
Exclusions
- Cases where a known previous positive test has been obtained within the last eight weeks
- Patients less than two years old at date of admission.
For guidance on testing procedures for C. difficile see the Public Health Laboratory Network. Clostridium difficile infection laboratory case definition.
Calculation of CDI rates
The following formula should be used to calculate the rate of C. difficile infection in acute inpatient hospitals:
| Numerator: | Patient episodes of hospital identified CDI (total hospital CDI cases) x 10,000 |
| Denominator: | Number of patient days |
A hospital’s CDI rate should be calculated routinely as per the local surveillance plan. For example, on a monthly or quarterly basis to enable early outbreak detection and ongoing evaluation of the local infection control program.
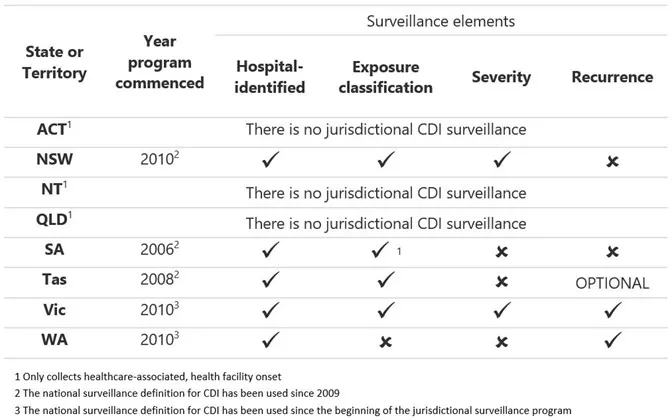
State CDI surveillance programs
Current state and territory CDI surveillance programs are summarised below:
National monitoring and reporting
The Commission has monitored the national burden of Clostridioides difficile infection (CDI) in Australian public hospitals since 2016. This work has led to a better understanding of CDI acquisition in hospitals and in the community in Australia and has helped to inform the development of measures to prevent and limit disease spread.
Data snapshots
- CDI data snapshot report 2022 and 2023
- Clostridioides difficile infection - 2020 and 2021 Data Snapshot
This report summarises the burden of CDI in Australian public hospitals during 2020 and 2021.
Collecting and using infection surveillance data
Understanding where and why infections occurs in hospitals is a crucial part of preventing infections. Along with routine surveillance, hospitals need to analyse their data in a meaningful way so they can see what is working well and where more support, different approaches or extra resources may be needed.
To help with this, we have created the following resources to support how hospitals can better interpret and use their surveillance data as part of ongoing quality improvement in infection prevention and control.