2026 National Model for Clinical Governance
The 2026 National Model for Clinical Governance (national model) aims to drive high-quality care and better outcomes for patients in Australian hospitals.
The national model is a short, simple, principles-based document that describes key actions and clarifies roles within health services to achieve high-quality care. It signals a strategic shift in how clinical governance is understood, led and embedded in all health services.
The model:
- elevates clinical governance to the highest level of organisational leadership and oversight, highlighting the crucial role of boards and executives in governing for high-quality care
- reshapes Australia’s approach to clinical governance, shifting the main focus from complying with accreditation requirements to building the culture of the organisation to one in which delivery of high-quality care is the core focus of everyone in a health service, every day.
The national model is accompanied by a practical guide to implementation and tools.
Go to the practical guide to implementation
Health services can use the guide to review their organisation’s clinical governance arrangements, identify gaps, develop an implementation plan, and monitor delivery of high-quality care.
The national model replaces the 2017 National Model Clinical Governance Framework.
Our Clinical Governance page has frequently asked questions about the model.
About the national model
Clinical governance establishes the conditions for high-quality care. It builds an environment and culture where everyone in a health service works together and with patients and consumers to deliver high-quality care.
The National Model for Clinical Governance (national model) provides updated national guidance on clinical governance that is clear, relevant and effective in helping health services to strive for consistently high-quality care.
Health service leaders can use the national model to review and strengthen their clinical governance systems and to identify and monitor what their organisation needs to achieve consistently high-quality care.
The national model provides a definition of high-quality care and describes the six foundations of clinical governance required to achieve this care:
- Leading systems and organisational culture
- Partnering with patients, carers and consumers
- Building a healthy workforce culture
- Enabling high-quality and integrated clinical practice
- Managing and reducing risk
- Using data for better care
Who this model is for
The national model is for public and private health services in the acute sector, including day hospitals.
It is primarily intended for health service board members and executives or equivalent who are responsible for directing and implementing clinical governance systems essential for high-quality care. At the same time, the national model is designed to be understood by all the workforce as everyone has a role in providing or supporting the delivery of high-quality care.
“When board members, executives and clinical leaders champion clinical governance as fundamental to achieving high-quality care, it sets the tone for the rest of the organisation.”
Professor Christine Kilpatrick AO, Board Chair, Australian Commission on Safety and Quality in Health Care
How to use the national model
Boards and executives (or equivalent) can use the model to govern, lead and plan for high-quality care through:
- building a shared language and understanding across the workforce of the definition of high-quality care and the six foundations of clinical governance required to support it
- designing systems and processes and shaping organisational culture to achieve consistently high-quality care
- enhancing accountability and clarifying roles and responsibilities
- guiding their approach to meeting safety and quality standards.
State and territory health departments and private hospital groups can use the national model to inform clinical governance systems and to shape detailed guidance for health services.
“The national model provides a structured way for me to conduct a gap analysis with the board and executive team to sharpen our clinical governance strategy – to visualise and articulate where we need to be.”
Lynne Walker, Chief Executive Officer, Perth Clinic, Western Australia
Implementing the national model
The national model is a principles-based document. Health services can apply the six foundations of clinical governance in a way that meets the needs of their organisation, no matter their size, type or location. An implementation guide offers practical steps for how health services can adapt the model.
Applying the national standards with purpose
The national model describes the systems, structures and culture for effective clinical governance in health services. As a principles-based document, the national model supports health services to review and strengthen their clinical governance arrangements and address the requirements of both the current and next edition of the National Safety and Quality Health Service (NSQHS) Standards. The six foundations of clinical governance will form the structure of the Clinical Governance Standard in the third edition.
Boards and executives should use the six foundations of clinical governance to check that their organisation’s strategy, systems and culture are aligned to deliver care that is consistently high quality and improving, no matter which safety and quality standards are in place.
The national model guides health services’ approach to applying NSQHS Standards in a meaningful way. By orienting every role and every system in the organisation to focus on high-quality care, and allocating resources to enable effective action, everyone in a health service can be confident that standards are being met every day – not just during accreditation assessments.
This fact sheet describes what the new national model means for assessment to the National Safety and Quality Health Service (NSQHS) Standards.
About clinical governance
What is clinical governance?
Clinical governance is central to providing the best possible outcomes for patients. It is the combination of organisational culture, systems and structures that enables everyone in a health service to deliver care that is consistently high quality and improving.
Effective clinical governance means that boards, executives, clinical leaders and the workforce are clearly accountable to patients and the community for providing high-quality care – care that is person-centred, safe, effective, accessible and integrated, provided in a way that is equitable, efficient and sustainable.
When done well, clinical governance builds trust across a health service. Patients experience care that better meets their needs. The workforce is confident that their organisation backs them with the right culture, structures, support and leadership to provide consistently high-quality care. Boards and executives have the oversight and tools they need to realise their strategy for achieving high-quality care.
Public inquiries into suboptimal care show that weak clinical governance can result in normalisation of poor care, ignored patient concerns, a culture of blame, a disengaged workforce, and overemphasis on legal and financial matters at the expense of care quality and patient outcomes.
Good governance
Corporate governance refers to the systems that direct and control – or govern – an organisation, including financial and legal functions.
Clinical governance and corporate governance are interdependent in a health service. Every board member and executive needs to understand that the core business of a health service is providing high-quality care, and that financial and operational decisions determine how resources are allocated to deliver that care.
“There is no corporate governance without clinical governance, because we are in the business of providing clinical care.”
Adjunct Professor Frank Tracey, Chief Executive, Children’s Health Queensland
Clinical governance for digitally enabled care
Robust clinical governance is needed for all types of care, whether delivered face to face or digitally enabled. Digitally enabled care includes virtual care, remote monitoring, and decision-making supported by artificial intelligence. Governance structures and systems must adapt to allow for changes in digitally enabled models of care, clinical workflows and technical requirements.
Clinical governance systems and frameworks must continue to evolve to harness the benefit of digitally enabled care – such as enhanced diagnostic accuracy, seamless information exchange across settings and support for personalised care – while safeguarding the safety and quality of care for patients.
High-quality care
The central aim of clinical governance is to deliver care to patients that is consistently high quality and improving. The Commission defines high-quality care as person-centred, safe, effective, accessible and integrated, provided in a way that is equitable, efficient and sustainable (Figure 1).
Cultural safety, as determined by Aboriginal and Torres Strait Islander people, is necessary for high-quality care. Cultural safety must be embedded in each domain of high-quality care to improve health outcomes for Aboriginal and Torres Strait Islander people.
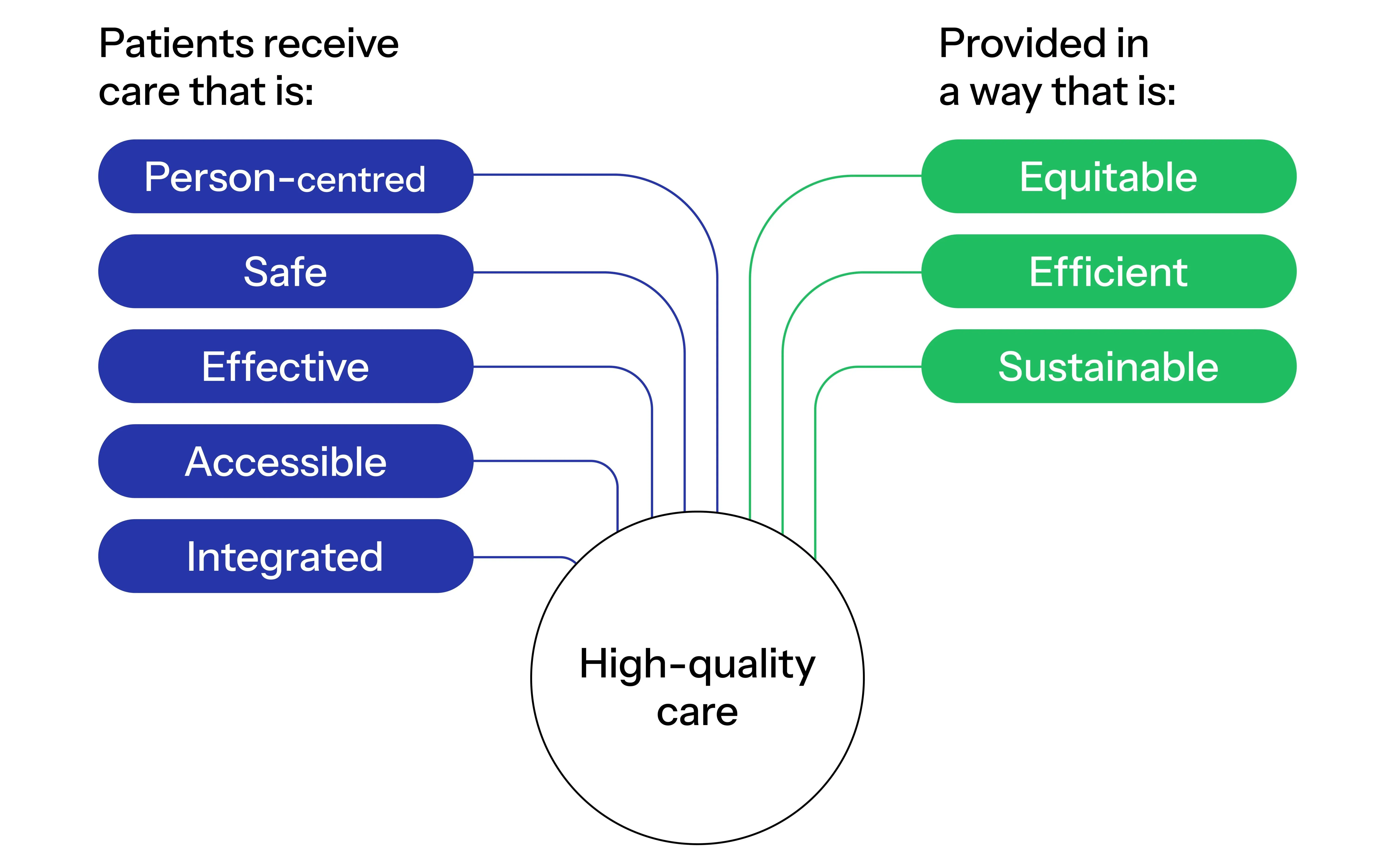
Figure 1: Diagram of domains of high-quality care. High-quality care is when patients receive health care that is: person-centred, safe, effective, accessible and integrated, and provided in a way that is: equitable, efficient and sustainable.
Person-centred | Respects the person receiving care, their family and carers, and responds to the person's preferences, needs and values |
Safe | Minimises risks of physical, psychological, psychosocial and cultural harms and factors that can contribute to actual of potential injury to the person receiving care |
Effective | Evidence-based and results in outcomes that benefit the person receiving care |
Accessible | Delivered at the right time and the right place |
Integrated | Coordinated and continuous within and between all parts of the healthcare system and other care settings and throughout the person's healthcare journey |
Equitable | Provides quality care to all people while responding to the needs of different groups to minimise differences in outcomes |
Efficient | Minimises cost and waste while achieving the best possible outcomes for people |
Sustainable | Minimises environmental impact and reduces emissions while achieving the best possible outcomes for people |
Roles in supporting high-quality care
Everyone in a health service – whether directly or indirectly involved in patient care – is responsible for achieving consistently high-quality care for every patient. To be effective, clinical governance needs to involve the board, executive and the workforce at all levels in a health service (Figure 2). Engagement and partnerships with patients, carers and consumers are critical to achieving high-quality care and better patient outcomes.
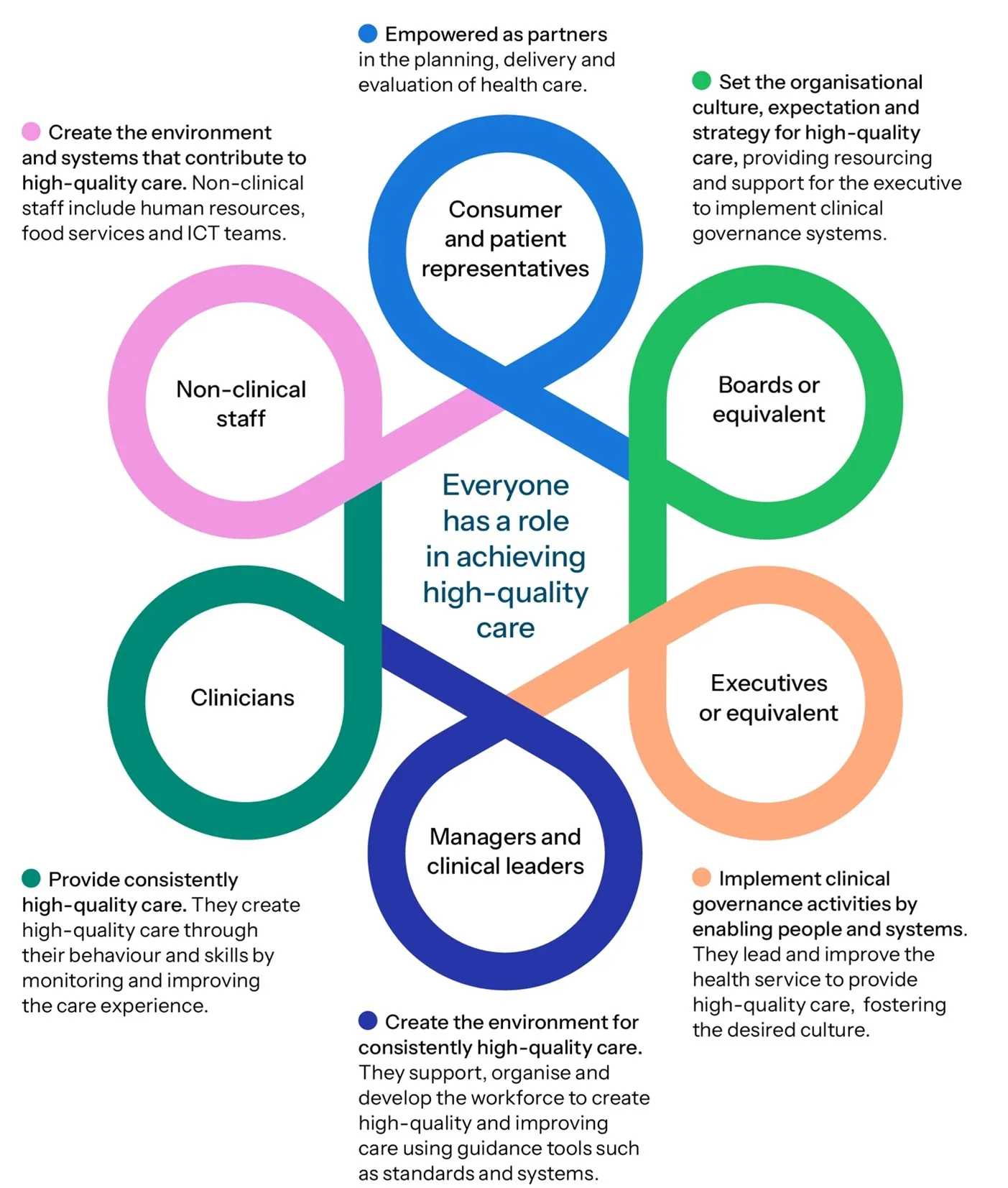
Figure 2: Diagram of roles supporting high-quality care in a health service. Everyone has a role in achieving high-quality care. Consumer and patient representatives are empowered as partners in the planning, delivery and evaluation of health care. Boards or equivalent set the organisational culture, expectation and strategy for high-quality care, providing resourcing and support for the executive to implement clinical governance systems. Executives or equivalent implement clinical governance activities by enabling people and systems, they lead and improve the health service to provide high-quality care, fostering the desired culture. Managers and clinical leaders create the environment for consistently high-quality care, they support, organise and develop the workforce to create high-quality and improving care using guidance tools such as standards and systems. Clinicians provide consistently high-quality care, they create high-quality care through their behaviour and skills by monitoring and improving the care experience. Non clinical staff create the environment and systems that contribute to high-quality care, non-clinical staff include human resources, food services and ICT teams. (This illustration has been adapted from an Australasian Institute of Clinical Governance resource – ‘I take responsibility’)
“Our CEO promotes all the time that our vision of best care is everyone’s business. You may not be providing direct clinical care, but you’re still providing best care, and everything you do contributes to providing best care.”
Alison Rule, Director Best Care Governance Compliance and Assurance, Western Health, Victoria
A note about patients and consumers
This model uses the term ‘patient’ for the person receiving care. It uses ‘consumer’ when referring to a consumer advocate or representative involved in clinical governance activities.
The six foundations of clinical governance
Clinical governance is the set of organisational systems aimed at supporting health services to deliver high-quality care. In this national model, these systems are structured into six foundations of clinical governance (Figure 3) that, when combined, underpin an organisational approach to delivering consistently high-quality and improving care.
The six foundations are connected and interdependent. As a health service’s priorities change, continuous monitoring, evaluation and improvement are required to check that activities are aligned with each foundation and achieve the purpose of providing consistently high-quality care.
Of the six foundations, leadership is a critical enabler of effective clinical governance. The board and executive provide clear strategic direction while creating an organisational culture in which there is leadership and accountability for providing high-quality care at all levels of the organisation.

Figure 3: Diagram of the six foundations of clinical governance and high-quality care. 1: Leading systems and organisational culture. 2: Partnering with patients, carers and consumers. 3: Building a healthy workforce culture. 4: Enabling high-quality and integrated clinical practice. 5: Managing and reducing risk. 6: Using data for better care.
Cultural safety for Aboriginal and Torres Strait Islander patients and health service staff
All foundations of clinical governance emphasise that cultural safety is essential in achieving high-quality care for Aboriginal and Torres Strait Islander patients and communities and in creating and maintaining a safe environment for Aboriginal and Torres Strait Islander health service staff.
Good practice and warning signs
The foundations of clinical governance set out key examples of good practice. The examples are not a complete list – rather they are designed so that health services can assess their performance in each foundation area. Each foundation also includes warning signs that can alert boards and executives to weaknesses in their clinical governance systems.
1. Leading systems and organisational culture
Leadership of a health service’s systems and organisational culture is central to how care is delivered and the outcomes of that care.
Inquiries into safety and quality failings in health services have highlighted that leadership actions – or lack of action – have a major impact on the culture of a health service and how it operates. Ineffective systems and negative organisational culture contribute to suboptimal care, poor staff morale and higher costs, while robust systems and positive organisational culture are associated with a satisfied and motivated workforce and better patient outcomes.
The board and executive are accountable for establishing, maintaining and continually improving systems for high-quality care. They set the strategy and culture for high-quality care, and support the workforce and patients, carers and consumers to achieve better patient outcomes and experiences. The board and executive have a legal duty to provide a psychosocially safe environment for the workforce and patients.
What good practice looks like
| Key examples |
|---|
|
Warning signs
- Board meeting agendas have a disproportionate focus on legal and financial matters without due consideration of clinical governance.
- There is high turnover in key leadership roles.
- The board does not engage with clinical issues, e.g. the board rarely or never hears from clinicians and there are no board directors with clinical backgrounds.
- The board, executive and workforce do not reflect the community they serve.
- Responsibility for digital tools is siloed within Information and Communications Technology (ICT) functions and is not integrated with clinical governance systems.
2. Partnering with patients, carers and consumers
Partnering with consumers in clinical governance – and with patients in their own care – is critical to achieving high-quality care and contributes to better outcomes and experiences for patients, carers and consumers.
Governance systems at all levels of the health service enable patients, carers and consumers to shape their care. The board and executive lead systems that build a culture of person-centred care so that everyone in a health service partners with patients, carers and consumers to provide or support the delivery of high-quality care.
What is person-centred care?
Person-centred care is health care that respects the patient, their family and carers, and responds to the person’s preferences, needs and values.
Person-centred care is equitable, culturally safe and free from racism and all other forms of discrimination. Patients, carers and consumers are treated with dignity, respect and kindness.
What good practice looks like
| Key examples |
|---|
|
Warning signs
- Consumers are engaged to satisfy representation requirements for committees rather than to meaningfully inform clinical governance decisions.
- Patient-reported measures and outcomes are not monitored or, if monitored, areas for improvement are not identified or acted on.
- There are consistently low scores in patient experience surveys. Patient and consumer feedback is not acted on.
- The organisation fails to recognise diverse cultures, identities and experiences and to tailor responses and models of care to meet patients’ unique needs.
3. Building a healthy workforce culture
A supported, engaged and empowered workforce is essential for delivering high-quality care and improving patient outcomes. A positive workforce culture in which staff feel respected, valued and safe to speak up for safety is a critical factor in boosting workforce morale and enabling staff to provide or support consistently high-quality care.
Constraints such as workforce shortages and turnover and fewer senior staff mean it is more important than ever to build and support an effective and engaged workforce.
Many factors contribute to building and maintaining a workforce culture in which all staff feel responsible for the care provided and feel that they can raise issues. These factors include a physically, psychosocially and culturally safe workplace, effective supervision, development and performance management systems, management of workload and adequate staffing.
What good practice looks like
| Key examples |
|---|
|
Warning signs
- There is inadequate board oversight of workforce indicators, such as engagement surveys, feedback about cultural safety, retention rates and absenteeism.
- Workplace culture issues, such as low response rates to staff surveys and poor engagement with safety culture questions, are not recognised as risks to patient safety.
- The workforce is not encouraged to report problems and does not feel empowered to make change to improve outcomes.
- The organisation has a high priority on meeting financial targets at the expense of workforce wellbeing and quality of care.
- Digital health systems do not support clinical workflows, leading to workarounds and inefficiency.
4. Enabling high-quality and integrated clinical practice
The primary purpose of a health service is to provide clinical care to achieve the best possible patient outcomes. Patients are likely to have the best outcomes when their clinical care respects their needs and preferences, is informed by the best available evidence, and is integrated across clinical care providers and settings, both in the health service and in the community, including in general practice.
Clinicians are enabled to provide care that achieves the best possible outcomes for patients across the continuum of care. They use insights gained from data to improve care. Clinicians communicate clearly and respectfully and work collaboratively. Clinicians contribute to, and participate in, the organisation’s clinical governance systems. Leaders and managers create the systems and environment that support clinicians to provide consistently high-quality care.
What good practice looks like
| Key examples |
|---|
|
Warning signs
- There is inadequate use of comparative data on clinical performance, e.g. how healthcare use, clinical outcomes and patient experiences compare with similar organisations or trends over time.
- The organisation tolerates poor outcomes with no clear improvement actions or systematic monitoring of their effectiveness.
- There are problems in the culture of escalation – e.g. junior staff are hesitant to raise concerns and have variable access to senior clinician support; there is a tendency to minimise or dismiss red flags instead of triggering escalation pathways.
- There is a lack of systems and structures that allow clinicians to raise concerns with management.
- Digital solutions are implemented before the clinical problem is clearly defined or are used to replicate paper-based workflows rather than improve care.
5. Managing and reducing risk
Health services are, by their nature, high-risk environments. A strategic approach to risk management informs monitoring, planning and allocation of resources across all parts of the organisation. Risk management involves oversight of clinical, financial, digital, operational and strategic risks, because all affect each other and the quality of care delivered. It also involves review and analysis of risks to look for trends and drive improvement.
Effective risk management requires systems and a culture in which everyone in a health service understands how the organisation defines risk and is accountable for identifying circumstances in which patients or the workforce could be harmed and acting to prevent or control those risks. The health service promotes a safety culture that allows people to openly share lessons from safety investigations, and to contribute to responses to reduce risk. Risk management systems need to be robust and adaptable as new technologies and digitally enabled health care evolve.
What good practice looks like
| Key examples |
|---|
|
Warning signs
- Clinical care risks emerge ‘without warning’ – the board spends more time reacting to emergencies than on anticipating and addressing potential risks.
- There is a focus on individual incidents rather than identifying patterns or system issues.
- Excessive reporting of risks dilutes the focus on key risks and leads to a significant reporting burden.
- There is a failure to respond to incident reports, complaints and suggestions for improvement from the workforce.
- The organisation implements major programs of work without a risk-based approach.
6. Using data for better care
Collecting, analysing and acting on data about health service systems and performance, patient and workforce experience and patient outcomes is fundamental to providing high-quality care. Data are key to a planned and systematic program for continuous improvement across the health service.
Responsive governance is needed to use findings across the health service to inform learning, improvement and accountability. The board and executive champion a data-driven improvement culture by making data-informed decisions and providing information to all who need it.
High-quality data are used to identify areas for improvement and to provide feedback to the workforce to prompt behaviour change.
Insights from multiple data sources (quantitative and qualitative performance, experience and outcome measures, and patient and workforce feedback) are triangulated to provide a deeper understanding of the quality of health care and the impact of efforts to improve care. The organisation learns from other health services and sectors to improve their systems and quality of care.
What good practice looks like
| Key examples |
|---|
|
Warning signs
- A compliance mindset leads to excessive data collection (‘drowning in data’). There is a high reporting burden but lack of flexibility to respond to key risks and emerging issues.
- Data reports to the board are high on detail and lack insights, key messages and visualisations.
- The board and executive focus on positive data rather than pursuing data that reveal inconvenient truths, missing opportunities for improvement.
- Security controls do not keep pace with increasing volume and sources of data, resulting in data breaches.
Glossary
Accreditation A formal program where trained independent reviewers assess evidence of implementation for specified standards. In this document, the relevant standards are the National Safety and Quality Health Service (NSQHS) Standards.
Artificial intelligence Computer systems able to perform tasks that normally require human intelligence, such as visual perception, speech recognition, decision making and translation between languages.
Board or equivalent Directors (or key decision-makers/accountable people) whose responsibilities include governing, directing and monitoring a health service’s business, affairs and operations, including overall organisational performance and compliance.
Carer A person who provides personal care, support and assistance to another individual who needs it because they have a disability, medical condition (including a terminal or chronic illness) or mental illness, or they are frail or aged. An individual is not a carer merely because they are a spouse, de facto partner, parent, child, other relative or guardian of an individual, or live with an individual who requires care. A person is not considered a carer if they are paid, a volunteer for an organisation, or caring as part of a training or education program. For Aboriginal and Torres Strait Islander people, there may be a collective approach to carer responsibilities.
Clinical governance Clinical governance is central to providing the best possible outcomes for patients. It is the combination of organisational culture, systems and structures that enables everyone in a health service to deliver care that is consistently high quality and improving. Effective clinical governance means that boards, executives, clinical leaders and the workforce are clearly accountable to patients and the community for providing high-quality care – care that is person-centred, safe, effective, accessible and integrated, provided in a way that is equitable, efficient and sustainable.
Clinician A trained health professional who provides direct clinical care to patients. Includes registered and non-registered practitioners, nurses, midwives, medical practitioners, allied health professionals, paramedics and other professionals who provide health care, and students who provide health care under supervision.
Co-design A process where people who are traditionally considered experts in a field work in partnership with patients, consumers or other users to design a policy, process, service or service improvement.
Consumer A consumer advocate or representative who provides a consumer perspective, contributes consumer experiences, advocates for the interests of current and potential health service users, and takes part in decision-making processes.
Corporate governance The framework of rules, relationships and processes that directs and controls the overall direction of an organisation. It includes clinical governance, financial and legal functions, and stakeholder accountability.
Credentialing A process that verifies the qualifications and experience of a clinician to determine their ability to provide safe, high-quality healthcare services within a specific healthcare setting and role.
Cultural safety Cultural safety is determined by Aboriginal and Torres Strait Islander individuals, families and communities. Culturally safe practice is the ongoing critical reflection of health practitioner knowledge, skills, attitudes, practising behaviours and power differentials in delivering safe, accessible and responsive health care free from racism.
Data sovereignty Indigenous data sovereignty is the right of Aboriginal and Torres Strait Islander people, communities and organisations to maintain, control, protect, develop and use data as it relates to them.
Digital health The use of technology to help Australians live healthier lives with greater control and better access to their information. It includes My Health Record, electronic prescriptions and telehealth.
Digital health literacy The ability to access, understand, critically evaluate, and use digital tools and technologies to make informed health decisions and engage effectively with health services.
Digitally enabled care The appropriate integration and application of digital health in clinical settings to deliver, augment or coordinate patient care.
Environmentally sustainable health care Health care that minimises environmental impact and reduces emissions while providing high-quality care.
Equity The absence of unfair, avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically or geographically or by other dimensions of inequality (e.g. sex, gender, ethnicity, disability or sexual orientation).
Evidence-based practice Health care that integrates the best available research evidence with clinical expertise and the patient’s unique values and circumstances.
Executive or equivalent The executive team, or key decision-makers/accountable people, who manage the day-to-day operations of the organisation, its people and resources. It is headed by the chief executive officer (or equivalent), who implements the strategy approved by the board.
Foundations of clinical governance A set of organisational systems that enable health services to deliver high-quality care.
High-quality care Health care that is person-centred, safe, effective, accessible and integrated, provided in a way that is equitable, efficient and sustainable.
Integrated care Where all parts of the health system work together to deliver person-centred care that is seamless, comprehensive, coordinated and efficient across the continuum of care.
Just culture A just culture looks beyond human error as a root cause to identify system-based improvements that address contributing factors across all levels of the organisation.
Learning culture An environment that actively encourages curiosity, growth and knowledge sharing, in which everyone feels empowered to ask questions, learn from mistakes, and discuss ways to improve care.
Lived experience Someone with personal experience of ill-health, including mental, chronic or acute illness.
Low-value care Care that provides little or no benefit, may cause patient harm, or yields marginal benefits at a disproportionately high cost.
National Safety and Quality Health Service (NSQHS) Standards Accreditation standards operated by the Commission as a quality assurance mechanism. The Standards test whether relevant systems are in place to ensure that expected standards of safety and quality are met.
Open disclosure An open discussion between a healthcare provider and a patient when things go wrong that have harmed or had the potential to cause harm to the patient. The discussion may include an expression of regret by the provider, an explanation of what happened and its consequences, and steps to prevent it happening again.
Organisational culture A set of values, expectations, formal and informal practices, and behaviours that define the unique organisational environment. ‘The way things are done around here.’
Patient A person receiving health care.
Patient outcome The status of a patient that is wholly or partially attributable to an action, agent or circumstance.
Patient-reported experience and outcome measures Information collected directly from patients about their experience of health services, and the outcomes of health services.
- Patient-reported experience measures (PREMs) include patients’ views and observations on matters such as the accessibility and physical environment of services and aspects of the patient–clinician interaction.
- Patient-reported outcome measures (PROMs) are used to obtain information from patients on their health status such as overall health and wellbeing, the severity of symptoms such as pain, measures of daily functioning and psychological symptoms.
Person-centred care Health care that respects the patient, their family and carers, and responds to the person’s preferences, needs and values. Person-centred care is equitable, culturally safe and free from racism and all other forms of discrimination.
Priority group Specific population group at elevated risk of poorer health outcomes, including Aboriginal and Torres Strait Islander people, people with mental health conditions, those living in rural/remote or lower socioeconomic areas, and people identifying as gay, lesbian, bisexual, transgender or intersex.
Psychosocial safety Protection from hazards and risks in the workplace that may negatively influence mental health and emotional wellbeing.
Remote monitoring A system that uses software and medical devices to allow healthcare professionals to assess, monitor and care for patients virtually (such as in the home or remote areas).
Safety culture A culture in which everyone enables and cares for each other to adopt patient safety as part of routine business, with the wellbeing of the workforce and consumers at the centre.
Safe workplace A workplace that is physically, psychosocially and culturally safe.
Transitions of care A transition of care is when all or part of a person’s health care is transferred between care providers.
Triangulated data Using multiple sources of data, with awareness of their strengths and limitations for specific purposes (as in taking bearings from at least two reference points on a map).
Unwarranted healthcare variation Differences in clinical practices, treatments, or outcomes that cannot be explained by differences in patient needs, preferences or evidence-based guidelines.
Virtual care Any interaction between a patient and clinician, or between clinicians, occurring remotely with the use of information technologies.
Workforce All people working in a health service, including clinicians and any other employed or contracted, locum, agency, student, volunteer or peer workers.
References
- Australasian Institute of Clinical Governance. Creating an upward spiral of staff satisfaction and care quality – Together. Melbourne: AICG; 2024.
- Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- Australian Commission on Safety and Quality in Health Care. Review of the key attributes of high-performing person-centred healthcare organisations. Sydney: ACSQHC; 2018.
- Australian Commission on Safety and Quality in Health Care. The state of clinical governance in Australia: A needs analysis. Sydney: ACSQHC (unpublished).
- Australian Commission on Safety and Quality in Health Care. National Model Clinical Governance Framework. Sydney: ACSQHC; 2017.
- Australian Digital Health Agency. Clinical governance framework for digital health. Sydney: 2023.
- Australian Institute of Company Directors. Not-for-profit governance principles. 3rd ed. AICD; 2024.
- Balding C, Leggat S. Making high quality care an organisational strategy: Results of a longitudinal mixed methods study in Australian hospitals. Health Serv Manage Res. 2020;34(3):148–157. doi: 10.1177/0951484820943601.
- Bismark MM, Studdert DM. Governance of quality of care: a qualitative study of health service boards in Victoria, Australia. BMJ Qual Saf. 2014 Jun;23(6):474–82. doi: 10.1136/bmjqs-2013-002193.
- Braithwaite J, Herkes J, Ludlow K, et al. Association between organisational and workplace cultures, and patient outcomes: systematic review. BMJ Open. 2017 Nov 8;7(11):e017708. doi: 10.1136/bmjopen-2017-017708.
- DPV Health. Excellent Care. DPV Health’s Clinical & Quality Governance Framework. DPV Health; 2021.
- Flynn MA, Burgess T, Crowley P. Supporting and activating clinical governance development in Ireland: sharing our learnings. J Health Organ Manag. 2015;29(4):455–81. doi: 10.1108/JHOM-03-2014-0046.
- Fulop NJ, Ramsay AIG. Governance and Leadership. Elements of improving quality and safety in healthcare. Cambridge University Press; 2023. doi: 10.1017/9781009309578
- Department of Health and Human Services Victoria. Community services quality governance framework. State of Victoria; 2018.
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the quality chasm: A new health system for the 21st Century. Washington (DC): National Academies Press (US); 2001. doi: 10.17226/10027
- Kellner P, Tsering D, Ngo CL et al. Clinical governance definitions and themes from safety and quality and incidents. A rapid literature review and environmental scan. Sydney: ACSQHC (unpublished).
- Leggat SG, Balding C. Bridging existing governance gaps: five evidence-based actions that boards can take to pursue high quality care. Aust Health Rev. 2019 Apr;43(2):126–132. doi: 10.1071/AH17042.
- Leggat SG, Balding C. Effective quality systems: implementation in Australian public hospitals. Int J Health Care Qual Assur. 2018 Oct 8;31(8)1044-1057. doi: 10.1108/IJHCQA-02-2017-0037.
- Ngo CL, Kellner P, Tsering D et al. Contemporary definitions of quality health care: A rapid literature review. Sydney: ACSQHC (unpublished).
- Safer Care Victoria. Delivering high-quality care: Victorian clinical governance framework. Melbourne: State of Victoria; 2024.
- Scally G, Donaldson LJ. The NHS's 50 anniversary. Clinical governance and the drive for quality improvement in the new NHS in England. BMJ. 1998 Jul 4:317(7150):61–5. doi: 10.1136/bmj.317.7150.61.
- Western Health. Best Care Framework 2024. Melbourne: Western Health; 2024.